Gastroesophageal Reflux Disease (GERD) in Children
Gastroesophageal reflux disease (GERD) is an advanced form of acid reflux that leads to persistent symptoms such as vomiting, chronic heartburn, chest discomfort, and trouble swallowing.
Gastroesophageal reflux disease (GERD) is an advanced form of acid reflux that leads to persistent symptoms such as vomiting, chronic heartburn, chest discomfort, and trouble swallowing.
What is GERD?
Gastro-oesophageal reflux disease, or GERD, is a chronic, long-term digestive condition. It occurs when the contents of the stomach reflux back up into the oesophagus and cause discomfort to the child.
Babies younger than one year age frequently have GER. During the first three months of life, most newborns spit up a few times a day. Babies with GER don’t have any issues. By the time they are 12 to 14 months old, most babies outgrow this.
Additionally, it is typical for kids and teenagers between the ages of 1 and 19 to experience GER occasionally. They may not necessarily develop GERD as a result.
Gastro-oesophageal reflux disease, or GERD, is a chronic, long-term digestive condition. It occurs when the contents of the stomach reflux back up into the oesophagus and cause discomfort to the child.
Babies younger than one year age frequently have GER. During the first three months of life, most newborns spit up a few times a day. Babies with GER don’t have any issues. By the time they are 12 to 14 months old, most babies outgrow this.
Additionally, it is typical for kids and teenagers between the ages of 1 and 19 to experience GER occasionally. They may not necessarily develop GERD as a result.
When does GER become GERD?
Your baby, child, or teen might have GERD if:
Your baby, child, or teen might have GERD if:
- Your baby experiences symptoms like vomiting, gagging, coughing, or difficulty breathing that interfere with feeding.
- There is aversion to feed or excessive cring post-feed.
- If the infant is developing recurrent pneumonia or growth failure.
- Your baby shows signs of GER lasting beyond 1 year age.
- Your child is vomiting intermittently after eating food which is causing discomfort and aversion to food.
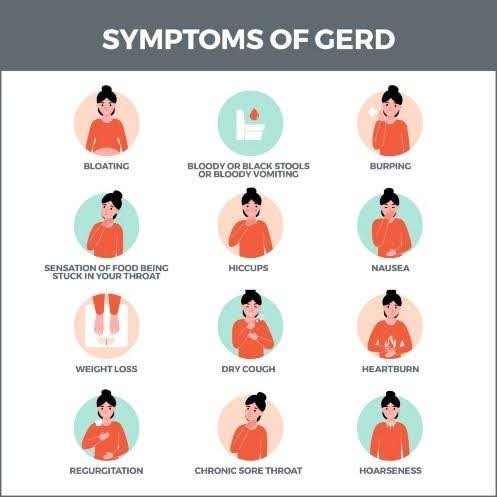
Common signs of reflux in children include:
- Heartburn
- Frequent burping
- Pain or difficulty in swallowing
- Regular nausea or vomiting, particularly after meals
- A sour or acidic taste in the mouth
- A sensation of stomach acid rising to the back of the throat
- Avoiding food or eating only small portions
Some symptoms may worsen when a child lies down after eating. Occasional reflux symptoms are normal, but frequent episodes could indicate GERD.

The lower esophageal sphincter, a ring of muscle, divides the esophagus from the stomach. If this ring doesn’t seal properly or relaxes at the wrong time, reflux symptoms occur. This permits the stomach’s acidic contents to return to the esophagus, the back of the throat, and occasionally the mouth or nose.
What Problems Can Happen?
Frequent reflux of stomach acid into the esophagus can cause:
Frequent reflux of stomach acid into the esophagus can cause:
- Breathing issues, such as choking, wheezing, or asthma
- Recurring pneumonia
- Cavities in the back teeth, even with proper brushing
- Esophagitis (inflammation and irritation of the esophagus)
- Esophageal damage, leading to difficulty swallowing
- Poor weight gain or unintended weight loss
How is GERD diagnosed?
To diagnose reflux in children, doctors typically perform a physical exam and discuss the symptoms. Keeping a record of foods that seem to trigger your child’s symptoms can help the doctor understand the issue better.
For children with persistent symptoms, a visit to a pediatric gastroenterologist (GI) may be necessary. In such cases, additional tests might include:
- Upper GI radiology study: A specialized X-ray that shows liquid backing up into the esophagus or narrowing of the esophagus.
- Upper GI endoscopy: A procedure where doctors use a tiny camera to examine the esophagus, stomach, and part of the small intestine. A small tissue sample (biopsy) may also be taken to check for other potential problems. Endoscopy although sounds scary but it is a very safe procedure in expert hands.

There are several ways to improve the symptoms of reflux in children.
Encourage your child to:
- Eat smaller, more frequent meals.
- Avoid foods and drinks that trigger symptoms, such as chocolate, caffeine, fatty or fried foods, spicy dishes, and peppermint.
- Refrain from eating late at night or lying down soon after meals.
- Maintain a healthy weight, as excess weight can sometimes contribute to reflux. A doctor can help create a suitable plan if needed.
If symptoms persist, your doctor may recommend medication. The course of treatment will be determined by your child’s age, overall health, symptoms and severity.
When Should I Call the Doctor?
Call your pediatrician or pediatric gastroenterologist if:
- Your baby is reflux is painful and leading to inadequate feeding.
- Infant is not gaining weight or developing recurrent cough.
In an older kid if:
- Having chest pain post food and aversion to food.
- Is very upset by the reflux.
- Isn’t growing as expected.
- Coughs, chokes, wheezes, or has trouble breathing.
- Vomits frequently after eating food.
- It’s affective sleep and daily routine activities.
Conclusion
Many babies who vomit will outgrow it by the time they are around 1 year old, as the lower esophageal sphincter gets stronger. For other children, medications and changes in diet and lifestyle can help reduce reflux, vomiting, and heartburn. Kids with reflux may be worried about their symptoms. Let them know that avoiding triggers and making simple changes can help them feel better.