Pediatric Inflammatory Bowel Disease (PIBD) is a chronic inflammatory condition of the intestines that poses significant health challenges in growing children. Unfortunately, this condition has significantly increased among the pediatric population of late.
Introduction
Inflammatory Bowel Disease causes chronic inflammation in the gastrointestinal (GI) tract; when this occurs in children (under 18 years of age) we call it PIBD. PIBD encompasses Ulcerative colitis (UC) and Crohn’s disease (CD) as its two main presenting forms. PIBD, be it UC or CD, is known for its remission and relapses which can be spontaneous, while on treatment, provoked by infections, or diet.
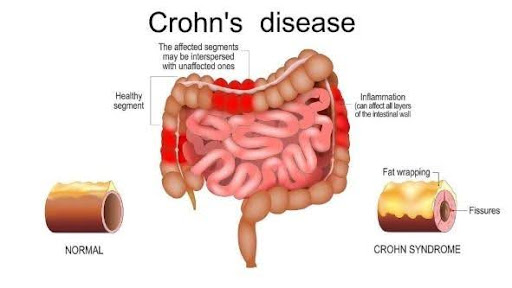
Crohn’s Disease is a type of PIBD that can affect any part of the gastrointestinal tract, from the mouth to the anus, though it most commonly involves the terminal ileum (a portion of the small intestine) and colon (large intestine). Unlike ulcerative colitis, which is restricted to the colon ( starting with the rectum, and extending variably in continuity, but only confined to the large intestine), CD is often characterized by discontinuous inflammation with intervening normal segments of the intestine termed ‘skip areas’.
Why Does Crohn’s Disease Occur?
The exact cause of PIBD (UC or CD) remains unclear. However, it is thought to result from a combination of genetic predisposition, immune system dysregulation, and environmental triggers. Those presenting before 6 years of age are included under the category Very Early Onset-IBD (VEO-IBD), where the possibility of genetic cause is highest. Pediatric patients often present with a stronger genetic predisposition compared to adults.
Key risk factors include:
Genetics: A family history of IBD increases the risk. Also, many genes are associated to be linked with causing IBD.
Environmental factors: Diet, gut microbiome changes, and infections may play a role.
Immune dysfunction: An abnormal immune response that can be either completely genetically driven (monogenic IBD) or triggered by gut dysbiosis (abnormal gut microbiota), contributes to inflammation.
In recent years, the change in diet from high fiber, natural foods to low fiber, processed items, refined items, added preservatives and frozen/stored items has contributed to the increase in PIBD.
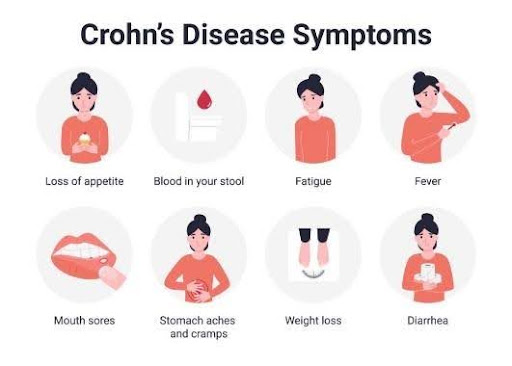
PIBD, although more common in the second decade, can present at all ages from infancy to 18 years. Common symptoms include:
Abdominal pain
Chronic diarrhea, sometimes with blood and mucus
Fatigue and malaise
Anorexia
Weight loss
Nausea, Vomiting
Delayed puberty
Extra-intestinal manifestations such as joint pain, skin rashes, jaundice, or eye inflammation may be seen in some.
When such symptoms are present for longer than 2 weeks, PIBD becomes an important diagnostic possibility. It requires timely evaluation and management as the disease can progress to complications like fistula, obstruction, perforation, and/or severe/resistant phenotype. Pediatric gastroenterologists are specialists in managing and caring for these children.
How is Crohn’s Disease diagnosed?
No single test is diagnostic of PIBD. Diagnosis is made by a combination of clinical presentation, inflammatory markers, endoscopy, histopathology, and imaging.
History and physical examination: In the initial visit, a detailed history and physical examination will be done for the child. Presenting symptoms, duration of illness, growth, pallor, clubbing, abdominal signs, etc. will be assessed.
Laboratory tests: Blood tests to check for anemia, inflammation (CRP, ESR, platelet count, protein, albumin), and nutritional deficiencies may be advised. Stool calprotectin is a very good test to assess baseline severity and for monitoring response to treatment.
Endoscopy and biopsy: Colonoscopy and upper GI endoscopy with tissue sampling are required. It helps to map the disease extent, as well as identify the type (UC or CD) of PIBD. It also provides tissue samples that can be used to differentiate from other close mimicking conditions like intestinal tuberculosis.
Imaging: Cross-sectional imaging like MR enterography or CECT enterography gives information regarding the disease extent, small bowel involvement, complications like fistula, stricture, etc.
There is no cure for Crohn’s disease yet, usually, these children are required to be on maintenance enteral nutrition or drugs for sustained remission, once induction is over. Pediatric gastroenterologists manage this condition with various medications and lifestyle changes, while continuously monitoring the disease. Treatment goals for pediatric Crohn’s disease focus on inducing and maintaining remission, promoting growth, and ensuring quality of life. The multidisciplinary approach includes:
Medications: These include medications like steroids, steroid-sparing immunosuppressants, immunomodulators, and biologics that help keep the inflammation under control. For active infections or complications, antibiotics or probiotics may also be prescribed.
Nutrition and diet: As discussed, processed foods and a Westernized diet with low fiber are not good for the gut. Crohn’s disease exclusion diet (CDED; more practical), or exclusive enteral nutrition (EEN) has been shown to produce remission as good as steroids in some studies.
Supplements in the form of iron, calcium, vitamin D, and vitamin B12 are usually given depending on the disease phenotype.
Lifestyle changes: Exercise, healthy foods especially rich in fiber, coconut water, avoiding unnecessary use of antibiotics, and avoiding stress promote good gut microbiome and help prevent flares and maintain remission.
Surgery: Surgery is only reserved for complications like strictures, fistulas, or abscesses and is not a part of first-line management in PIBD. Colectomy can completely cure ulcerative colitis.
Since chronic illness impacts mental health and the quality of life of the child and entire family; counseling and support groups are essential for children and their families. Hence a team approach with family/child at the center, along with a pediatric gastroenterologist, dietician, and psychologist (as required) will help the child to overcome his symptoms.
Living with Crohn’s Disease
Managing Crohn’s Disease is a lifelong process. For children, fostering adherence to treatments and regular follow-ups is critical. Encouraging open communication about symptoms and challenges helps build resilience. With current and further advancements in treatment, many children with CD go on to lead fulfilling lives. All these children need is a team that truly cares for them and is motivated to give them the best quality of life.
Conclusion
Pediatric Crohn’s Disease, though challenging, can be managed effectively with timely diagnosis and a holistic approach. Awareness among parents and caregivers is vital to recognize early signs and seek specialist care. With current management strategies, the goals of disease remission and providing the best quality of life can be achieved in nearly all children with PIBD.
Our healthcare specialists are equipped with the knowledge and skills to provide you with the support you require. From consultation to diagnosis to treatments, our experts are dedicated to helping you.